

Introduction
Dose adjusted (DA) EPOCH-R is an intensive outpatient infusional regimen, that incorporates intrathecal (IT) methotrexate to treat patients with aggressive B-cell lymphoma including HIV associated aggressive B-cell lymphoma, double-hit lymphoma (DHL), primary mediastinal B-cell lymphoma (PMBCL), Burkitt's lymphoma (BL) ineligible for intensive therapy, and gray zone lymphoma (GZL) with features in between BL and diffuse large B-cell lymphoma (DLBCL). We aimed to evaluate non-trial, progression-free survival (PFS) and overall survival (OS) of Manitoba patients treated with DA-EPOCH-R, assess the role of prophylactic IT chemotherapy and toxicities.
Methods
Patients in MB approved to receive DA-EPOCH-R were identified through the CCMB Provincial Oncology Drug Program (PODP) database. Patients were included if they were older than 17 years, received at least 1 cycle of DA-EPOCH-R and with a diagnosis of HIV associated aggressive B-cell lymphoma, DHL, PMBCL, BL ineligible for more aggressive therapy, or GZL. All other diagnoses were excluded. Baseline demographic data, treatment characteristics, treatment responses, and treatment toxicity were collected. The primary endpoints of the study were progression free survival (PFS) and overall survival (OS). PFS was the time interval between the date of diagnosis to date of progression, last follow-up, or death from any cause. OS was the time interval between date of diagnosis to date of death by any cause, or last follow-up. The study was approved by the University of Manitoba Research Ethics Board and the CancerCare Manitoba Research Resource Impact Committee.
Results
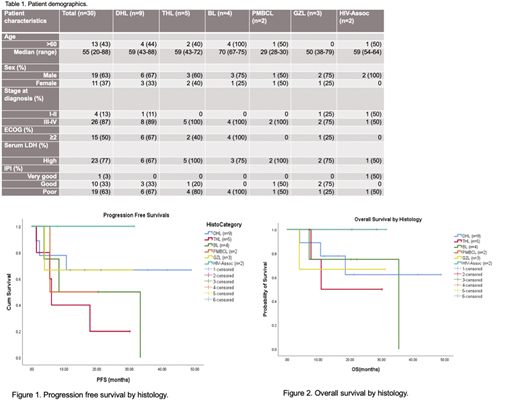
A total of 40 patients were approved for DA-EPOCH-R between 2013 and 2019. 10 of these patients were excluded. 4 patients never received the therapy, 4 patients were treated in the relapsed setting, and 2 patients had histologies outside the inclusion criteria. Of the 30 patients included, 19 (63%) were male, 11 (37%) were female. The median age at diagnosis was 55 years (range 20-88). Our cohort was composed of DHL (n=9), triple hit lymphoma (THL, n=5), BL (n=4), GZL (n=3), and HIV-associated DLBCL (n=2). 87% (n=26) had advanced stage disease. By revised-IPI, 19 (63.3%) had poor prognosis (R-IPI ≥ 3). Response rate was 90%; CR 53.3% (n=16) and PR 37% (n=11). At a median follow-up of 25.3 months, the median PFS was 33.3 months and median OS was not reached. By histological subtype, median PFS was not reached in DHL, however THL, BL and PMBCL had worse median PFS (6.1, 8.4, and 5.6 months, respectively). Only 1 patient had CNS involvement at time of diagnosis. Of the patients with no documented CNS disease at presentation (n=29), none developed CNS involvement, including those who did not receive IT methotrexate. Median chemotherapy cycles per patient was 6 (range 1-6) and median IT treatment was 3 (range 0-6). 3 patients did not receive IT prophylaxis, and 2 stopped after 1 cycle due to intolerance. 56.7% (n=17) were able to undergo dose escalation beyond dose level 1, and 40% (n=T12) tolerated maximum dose level 3 or higher.77% of patients (n=23) experienced at least one adverse event of grade 3 or higher. 17 (57%) patients required blood transfusion at least once. 10 (33%) experienced neuropathy, 4 requiring vincristine dose reduction. 9 (30%) patients had febrile neutropenia complicating a total of 22 treatment cycles. 8 patients had grade 2-3 infectious complications.
Conclusions
While the real-world survival data for patients with DHL and HIV-associated lymphoma treated with DA-EPOCH-R are encouraging, those with THL, BL, and PMBCL did not attain durable response. Considering no patients (including those who did not receive IT chemotherapy) experienced CNS relapse, the role of IT chemotherapy needs to be further clarified.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal